
Tooth Resorption is an unfortunately common, painful, and under-diagnosed dental problem in pet cats. While advanced disease may be picked up on a thorough physical exam in a cooperative cat, early lesions are nearly impossible to catch without an anesthetized exam and x-rays. Likewise, while some cats with this disease will show obvious signs of pain like changes in appetite or attitude, most of the time when we diagnose the condition pet parents had no idea anything was wrong. This makes resorptive lesions a major reason why we recommend regular professional dental care for cats – if we don’t have the opportunity to diagnose the problem, your pet may well be living with pain.

What Is Tooth Resorption?
Resorptive lesions occur when specialized cells start eating away at the outer layers of the tooth, exposing the raw nerve endings in the dentin and eventually the pulp canal. Why this happens so commonly in cats is unknown, though it is the subject of active research. Current evidence suggests there are probably multiple causes. Sometimes the process appears to be initiated by the inflammation that inevitably results from poor oral hygiene, but there may be a genetic component that makes some cats more susceptible than others as resorptive lesions can occur even in otherwise healthy mouths. Regardless, the end result is usually painful, fragile teeth.
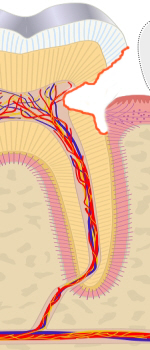
Each tooth is made up of a living pulp canal that contains the tooth’s nerves and blood supply. The pulp canal is covered with protective dentin, which makes up the majority of the tooth. The exposed surface of teeth is further covered with a protective layer of the hardest substance in the body – enamel. While enamel has no nerve endings and is essentially inert, the dentin it covers is filled with nerves. This is why a chipped tooth hurts but normal teeth don’t really feel anything.
Diagnosing Resorptive Lesions
Late-stage lesions like the ones pictured above may be diagnosed during a thorough physical in a cooperative cat. However, early lesions are often at or below the gumline, making them impossible to recognize without x-rays – even though they may already be causing significant pain. Likewise, many cats will only allow the most cursory of oral exams without anesthesia – and cats with this disease are often particularly uncooperative for understandable reasons. In one study of 228 clinically healthy cats 29% were found to have at least one lesion on x-rays. This means regular anesthetized exams with x-rays are the only real way to know if your pet is affected or not.
Furthermore, since the problem may be identified even in otherwise healthy mouths, and we don’t fully understand what triggers the disease, we have no way to try and prevent tooth resorption. This means being vigilant about regular exams and x-rays to screen for the problem is our best tool for keeping cat’s mouths healthy and comfortable.
Treatment
Since there is no way to reverse the process, treatment almost always involves extraction of the affected teeth. Since the disease leaves the teeth fragile and prone to breakage it can be quite difficult and time consuming to remove the entire tooth. Occasionally the process affects the root and begins replacing it with bone (known as Type 2 resorption), and in this circumstance a removal of the crown and closure of gingiva over the resorbing root may be sufficient. In all other cases, however, the entire fragile root needs to be removed to ensure the pet does not develop problems. This makes x-rays to confirm complete extraction absolutely essential.
Most cats who develop resorptive lesions will develop them on multiple teeth, and many eventually require full-mouth extractions to be comfortable. For this reason, whenever we diagnose and treat this problem a follow-up exam with x-rays is recommended to evaluate for new lesions. In cases where we find and treat a single lesion, we may recommend follow up at their next annual cleaning, but in more severe cases we usually recommend follow-up in 3 to 6 months.